


Case Interpretation | How to maximize the lumen benefit when emergency PCI is accompanied by left main bifurcation lesions?
Release time:
2024-11-27
The treatment strategy of left main bifurcation lesions has been a controversial topic in clinic. How to choose the optimal treatment strategy for emergency PCI? Does the choice among different devices help the surgeon more?
Introduction
The treatment strategy of left main bifurcation lesions has been a controversial topic in clinic. How to choose the optimal treatment strategy for emergency PCI? Does the choice among different devices help the surgeon more?
Today, the editor brings you this case sharing: How to achieve the best treatment effect when emergency PCI is accompanied by left main bifurcation lesions?
01 Patient Information
Basic information:
Sex: Male;
Age: 43 years old;
Weight: 80 kg;
Medical history data:
Chief complaint: sudden chest pain for 11 hours;
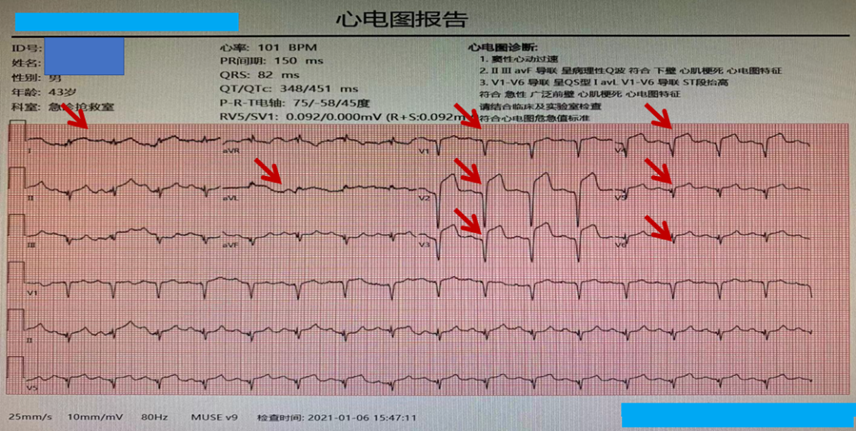
Present illness: The patient had chest pain after activity 11 hours ago, accompanied by profuse sweating, shortness of breath, and fatigue, which continued to fail to relieve. An electrocardiogram performed at the local hospital indicated “acute anterior wall myocardial infarction.”
Past history: A stent was implanted in the LAD due to angina six months ago, but the medication was not taken as required after the operation; He has a 7-year history of diabetes and is treated with oral metformin and glimepiride, but the blood glucose is poorly controlled; he has a history of hyperlipidemia for many years;
Personal history: Smoking for 30 years, with 40 cigarettes/day; occasional drinking;
Physical examination:
Clear mind and poor energy in semi-recumbent position;
BP: 124/94mmHg, P: 96bpm;
No abnormalities heard in the heart, lungs and abdomen, and no edema in both lower limbs;
Laboratory tests:
Cardiac color ultrasound: EF: 43%, left ventricular anterior wall motion amplitude decreased, no abnormalities in each cardiac chamber, valve, or aorta;
cTNI: 4.0ng/mL, MYO: 807ng/mL, CK-MB: 278ng/mL;
Blood glucose: 14.64mmol/L;
Admission examination:
Electrocardiogram: ST segment elevation in leads I, avL, V1-V6
Hospitalization
After admission, the patient’s chest pain continued to worsen, accompanied by profuse sweating and feeling of impending death, and had no response to loading-dose aspirin and clopidogrel. The chest pain was not relieved after nitroglycerin treatment, and morphine was given for sedation and analgesia, but the effect was still not significant. According to the patient’s clinical manifestations, a loading dose of Tirofiban was given and intravenous drip was maintained, and the chest pain symptoms were slightly relieved but still present. Emergency PCI was planned.
Primary diagnosis
1. Coronary atherosclerotic heart disease
1.1 Acute extensive anterior wall myocardial infarction
1.2 Cardiac function class I (Killip classification)
2. Type 2 diabetes
3. Hyperlipidemia
02 Coronary Angiography
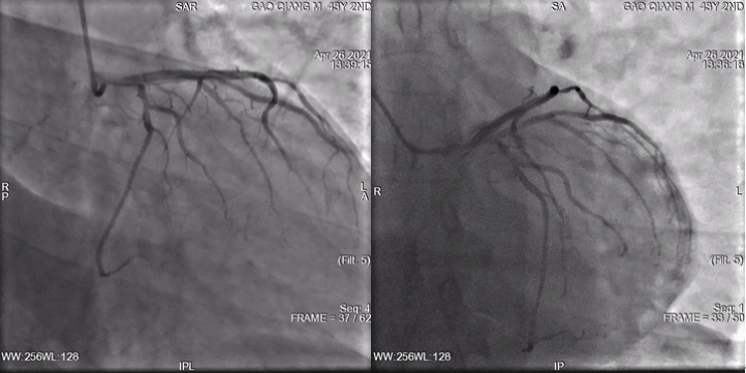
Right coronary angiography
Mild stenosis in the proximal RCA segment

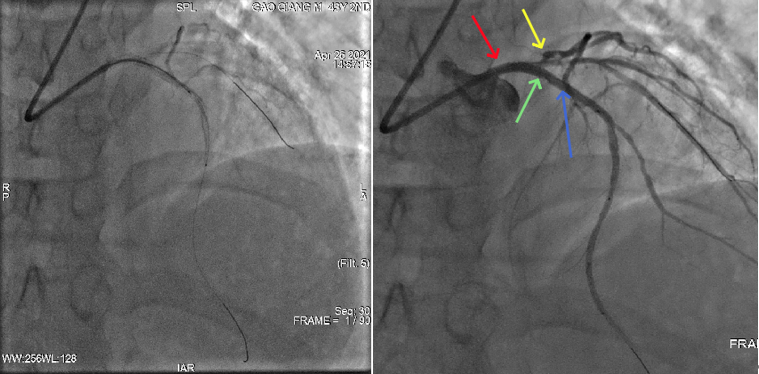
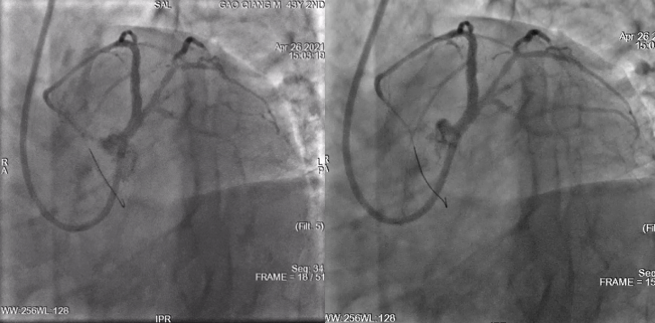
Left coronary angiography
Moderate to severe stenosis in the LM opening, no obvious abnormality in the original DES
Analytical judgment and response
Mild stenosis in the proximal RCA segment
Moderate to severe stenosis in the LM opening indicated infarction-related blood vessel, and emergency revascularization is planned;
The patient’s vital signs were stable, but considering the left main artery lesions and the patient’s young age, ECMO was implanted;
03 Surgical procedure
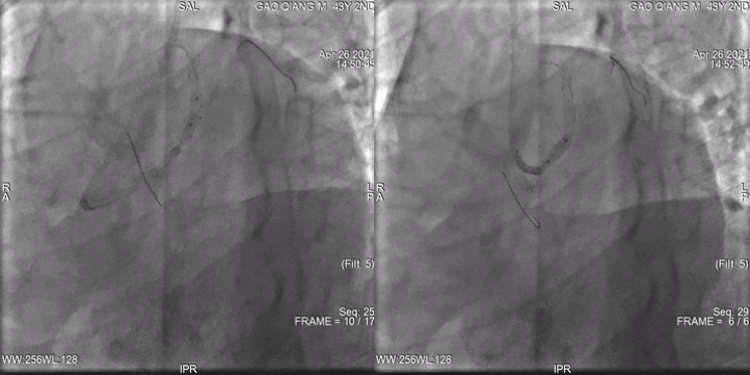
Pretreatment procedure
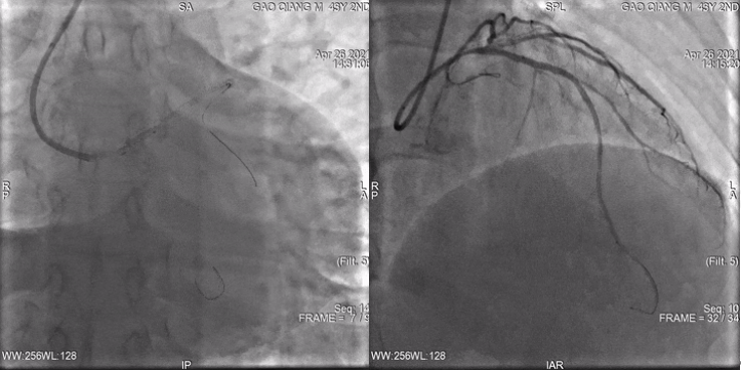
Under ECMO support, the left coronary artery was processed with radial artery approach and double GW, the guiding catheter EBU3.5 was selected, and a 2.5mm diameter balloon was used for pre-dilation treatment (12atm).
Immediate imaging after pretreatment

OCT intracavity imaging results showed that LM was severely narrow, LAD and LCX openings were basically normal
Key procedure I
A 3.5*16mm stent was implanted in the left main artery-anterior descending artery (expanded and released at 18-20 atm), and then a 3.5*10mm high-pressure post-dilatation balloon was used for POT treatment (expanded at 18-20 atm).
After the exchange of the guidewire, the KBI was engaged with the balloon, and the 3.5*10 high-pressure post-dilatation balloon was used to expand the KBI by 20atm pressure and then POT treatment was performed again (Re-POT).
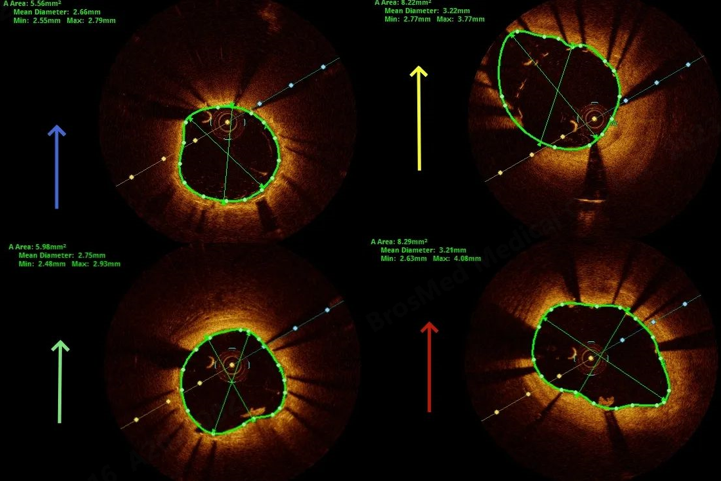
OCT intracavity imaging results showed that incomplete expansion and poor apposition of LAD-LM stent
Key procedure II
Poor apposition of the main branch stent in left main coronary artery disease can easily lead to in-stent restenosis, acute thrombosis in the left main coronary artery stent and other serious cardiovascular adverse events, affecting the patient’s prognosis and even endangering life.
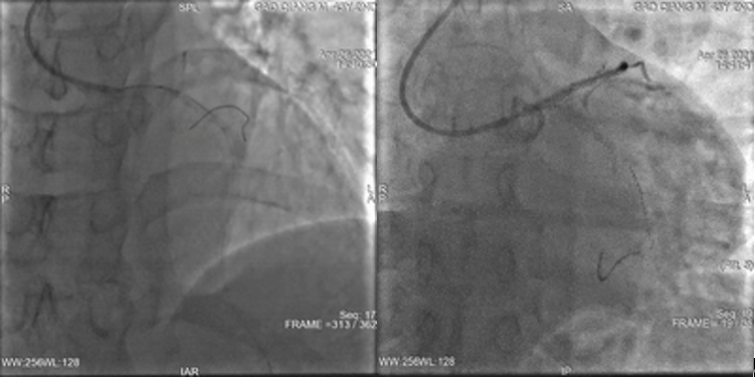
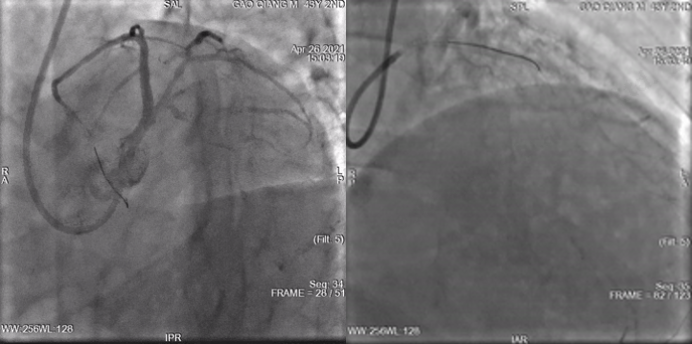
The POT™ balloon (3.5*10mm, expanded at 22-24 atm), with very short and round shoulder design for precise positioning and expansion, can optimize the stent implantation to fully apposition to the wall, so as to maximize the lumen area and better modify branch openings. Angiography showed immediate recovery of blood flow.
Immediate postoperative angiography
Case Summary
Case characteristics
This patient had undergone stent implantation for coronary heart disease, but suffered myocardial infarction again due to non-standard postoperative medication. Left main coronary artery disease has an extremely high mortality rate and extremely poor prognosis, which poses a severe challenge to the comprehensive treatment level of the medical team.
Preoperative key points assessment
Under the protection of ECMO implantation, this patient used endovascular OCT imaging to accurately evaluate the vascular condition, and then underwent rapid single-stent treatment to complete revascularization.
Surgical points
Quickly complete revascularization and accurately implant the stent at the left main coronary artery disease, which must be accurate post-dilatation.
Device use points
As the exclusive balloon for POT and DOT technologies, the POT™ balloon has obvious advantages in the treatment of bifurcation lesions and is the best choice for POT technology.
The POT™ balloon is indicated for stent placement in bifurcation lesions and to improve the treatment of stent post-dilation. The extremely short balloon shoulder design enables precise positioning and expansion, ensuring that the stent is in full apposition to the wall. The unique balloon material makes the balloon have minimal compliance changes, thereby avoiding the dog bone phenomenon and reducing the damage to the surrounding normal blood vessels.
Clinical Cases

The treatment strategy of left main bifurcation lesions has been a controversial topic in clinic. How to choose the optimal treatment strategy for emergency PCI? Does the choice among different devices help the surgeon more?
2024-11-27

Vascular access is the lifeline for hemodialysis patients. Prolonging the service life of the access, guarding the “lifeline” of hemodialysis and ensuring the smooth flow of the “lifeline” are the top priority in maintaining the vascular access. The emergence of the scoring balloon brings the hope of improving patients’ dialysis access patency rate and reducing pain, and is expected to become a better choice for the treatment of arteriovenous fistula stenosis……
2024-11-27
The common symptoms of severe lower limb calcification include coldness, numbness and intermittent claudication in the lower limbs. In severe cases, there may be persistent pain and weakening or disappearance of dorsal foot artery pulsation, and gangrene may occur when the artery is completely occlusive. Calcified lesions destroy the normal blood vessel wall, causing uneven pressure on the blood vessel wall, thinning of some walls, and changes in hemodynamics, which can easily lead to fixed stenosis, thrombus, aneurysm, and aortic dissection.
2024-11-27
 of AVF")
Case Interpretation| Application of Tri-Wedge™ in Juxta-anastomotic Stenosis(JAS) of AVF
In the previous issue of case sharing, we presented a complex coronary intervention case, in which the Alveo HP Φ0.75 balloon, independently developed by BrosMed Medical, demonstrated excellent performance in crossing the lesion and dilation, showcasing exquisite craftsmanship of innovation.
2024-11-27
 Occlusion with Calcification Using Alveo HP Φ0.75 mm Balloon")
For acute occlusion with calcification in right coronary artery (RCA), neither PCI microcatheter nor 1.2/1.0 mm balloons can cross the lesion in emergency treatment??? What other device can be considered by operator in elective operation?
2024-11-27