


Case Interpretation | Outstanding Performance of Tri-Wedge™ in the 12atm Dilation of Severe Subclavian Vein Stenosis
Release time:
2024-11-27
Vascular access is the lifeline for hemodialysis patients. Prolonging the service life of the access, guarding the “lifeline” of hemodialysis and ensuring the smooth flow of the “lifeline” are the top priority in maintaining the vascular access. The emergence of the scoring balloon brings the hope of improving patients’ dialysis access patency rate and reducing pain, and is expected to become a better choice for the treatment of arteriovenous fistula stenosis……
Vascular access is the lifeline for hemodialysis patients. Prolonging the service life of the access, guarding the “lifeline” of hemodialysis and ensuring the smooth flow of the “lifeline” are the top priority in maintaining the vascular access. The emergence of the scoring balloon brings the hope of improving patients’ dialysis access patency rate and reducing pain, and is expected to become a better choice for the treatment of arteriovenous fistula stenosis……
In the last Tri-Wedge™ case sharing, we introduced a case of AVF anastomotic stenosis treated by Tri-Wedge™ to our readers, but central venous stenosis is also a common lesion in clinical practice, which also has high requirements for balloon passability and dilatability.
Today, we bring you a new case. Let’s take a look at the outstanding performance of Tri-Wedge™ in the left subclavian vein……
Case information
Patient information: female, 65 years old, 45kg
Visit time: June 13, 2023
Chief complaint: hemodialysis for more than 10 years, hemostasis difficulty at internal fistula of left forearm for more than 3 months
Present illness: The patient was found to have “polycystic kidney and polycystic liver showed by ultrasound examination; serum creatinine 800+umol/L; blood Hb 72g/L” more than 10 years ago,underwent “internal arteriovenous fistulation in the left elbow”, and began regular dialysis after the internal fistula was matured; since March, the patient had experienced hemostasis difficulty after puncture of the arteriovenous fistula in the left forearm, accompanied by repeated hemostasis difficulty in the vein after puncture of the fistula. Examination suggested “left subclavian vein stenosis”, so the patient was hospitalized several times to undergo PTA treatment, but the effect was not long-lasting, and hemostasis difficulty persisted. Therefore, the patient is now hospitalized.
Past history: hypertension for 10 years
Admission examination
Admission examinPhysical examination: Clear mind and chronic disease face; superficial lymph nodes of the whole body were not enlarged; clear breath sounds of both lungs, no dry or moist rales; regular cardiac rhythm, heart sounds S1 and S2 were of moderate intensity, S3 and S4 were not auscultated; the abdomen was soft, and the tenderness was noted at right upper abdomen, no rebound tenderness or mass; liver and spleen were not palpated below the costal margin, the gallbladder was not palpated, Murphy’s sign was negative, there was no percussion tenderness over kidney region, the bowel sound was normal, shifting dullness was negative; both lower limbs were not swollen, pathological signs were negative, left forearm internal arteriovenous fistula tremor was palpable, and the vessel was dilated.
Laboratory tests: Relevant examinations were completed after admission, [2023-06-13] hematology test + hs-CRP: hypersensitive C-reactive protein (whole blood): 296.4 mg/L↑; White blood cell count * (whole blood): 11.5×*10^9/L↑ Potassium * (serum): 3.28 mmol/L↓; Creatinine * (serum): 793 μmol/L↑;
Left internal fistula angiography: severe stenosis of left cephalic venous arch and subclavian vein, with multiple collateral circulation formation.
Multiple stenosis of left internal fistula cephalic vein outflow tract, with tumorous dilatation and localized wall roughness and calcification. Please combine with clinical manifestations.
Diagnostic result:
1. Stenosis of internal arteriovenous fistula;
2. Stage 5 chronic kidney disease;
3. Polycystic kidney;
4. Hemodialysis;
5. Secondary hyperparathyroidism;
6. Renal hypertension;
7. Renal osteopathy;
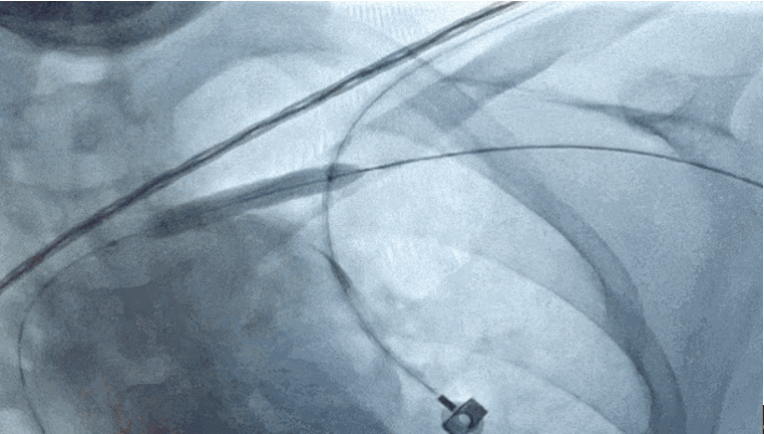
Preoperative angiography

Angiographic analysis suggested severe stenosis of left cephalic venous arch and subclavian vein, with multiple collateral circulation formation.
Surgical procedure 1
01
Balloon dilatation: the stenotic vessel was dilated using a 6*40 mm scoring balloon, and the stenosis could be dilated at a pressure of 12 atm
02
Stent implantation: A 11*50 mm covered stent was implanted after the procedure, which dilated the stenosis
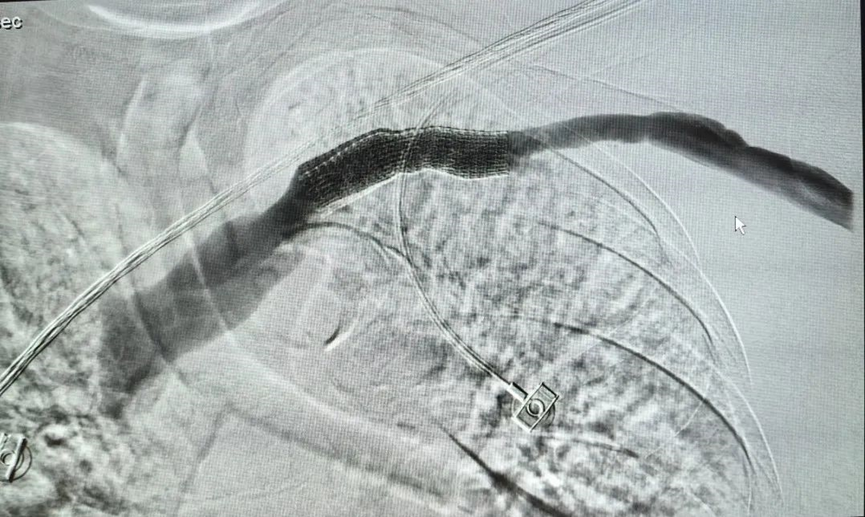 Postoperative | immediate angiography
Postoperative | immediate angiography
03
Comparison of preoperative vs. postoperative immediate angiography

Postoperative summary
Scoring balloon is a highly safe and effective option in the treatment of severe stenosis and “solid” lesions, with good dilatation effect.
The balloon has good passability and can pass through severe stenosis and even occlusive lesions. It can easily pass through corners of the cephalic vein, and can enter and exit the arterial sheath smoothly due to its small volume after decompression.
Scoring balloon dilatation can widen the narrowed passage with minimal pressure, and the patient feels less pain.
In this case, a 6*40 mm scoring balloon was used to pre-dilate a refractory stenosis, which realized subsequent smooth placement of coated stent and further widened the narrowed passage with post-balloon dilatation.
Clinical Cases

The treatment strategy of left main bifurcation lesions has been a controversial topic in clinic. How to choose the optimal treatment strategy for emergency PCI? Does the choice among different devices help the surgeon more?
2024-11-27

Vascular access is the lifeline for hemodialysis patients. Prolonging the service life of the access, guarding the “lifeline” of hemodialysis and ensuring the smooth flow of the “lifeline” are the top priority in maintaining the vascular access. The emergence of the scoring balloon brings the hope of improving patients’ dialysis access patency rate and reducing pain, and is expected to become a better choice for the treatment of arteriovenous fistula stenosis……
2024-11-27
The common symptoms of severe lower limb calcification include coldness, numbness and intermittent claudication in the lower limbs. In severe cases, there may be persistent pain and weakening or disappearance of dorsal foot artery pulsation, and gangrene may occur when the artery is completely occlusive. Calcified lesions destroy the normal blood vessel wall, causing uneven pressure on the blood vessel wall, thinning of some walls, and changes in hemodynamics, which can easily lead to fixed stenosis, thrombus, aneurysm, and aortic dissection.
2024-11-27
 of AVF")
Case Interpretation| Application of Tri-Wedge™ in Juxta-anastomotic Stenosis(JAS) of AVF
In the previous issue of case sharing, we presented a complex coronary intervention case, in which the Alveo HP Φ0.75 balloon, independently developed by BrosMed Medical, demonstrated excellent performance in crossing the lesion and dilation, showcasing exquisite craftsmanship of innovation.
2024-11-27
 Occlusion with Calcification Using Alveo HP Φ0.75 mm Balloon")
For acute occlusion with calcification in right coronary artery (RCA), neither PCI microcatheter nor 1.2/1.0 mm balloons can cross the lesion in emergency treatment??? What other device can be considered by operator in elective operation?
2024-11-27